by Kristian Hudson
Kristian Hudson is an implementation specialist with the Yorkshire & Humber Improvement Academy working with researchers and practitioners across the Yorkshire & Humber Applied Research Collaboration.
Implementation is a messy business. There are usually a million and one roadblocks between innovations that have been shown to work and them actually benefitting society. Most of the time, even when new health innovations are backed by mountains of scientific evidence, they experience the all too common ‘voltage drop’, whereby once they move into real world settings their effectiveness decreases over time.
For the last 20 years, the new discipline of Implementation Science has been trying to understand how to successfully ensure innovations make this journey from science to practice successfully
But even before Implementation Science became a recognised academic discipline scientists have been asking questions about implementation (Rogers for example put together his Theory of Diffusion in the 1960s (Rogers, 1995).
As an implementation specialist, whenever a clinician, nurse, policy maker, researcher, or anyone else trying to implement a project asks me how to implement it, I am fortunate to have implementation science research to draw from. However, as someone with experience of actually ‘doing’ implementation, I think there are some aspects of implementation which the science has so far struggled to capture. I am referring here in particular to the practical aspects of implementation, the golden ‘how to’. It is this information on ‘how to’ implement things that front line staff and practitioners are very keen for but who might struggle to get it from the implementation science literature.
What the implementation science literature is good at
Implementation science describes what implementation is. It is a science which makes implementation explicit and gives everyone a common language from which to talk about it. I can use the science to describe to people what implementation should look like. For example, I can show how it occurs in stages (e.g. exploration, preparation, initial implementation, implementation), and that there are things you might want to think about at each stage.
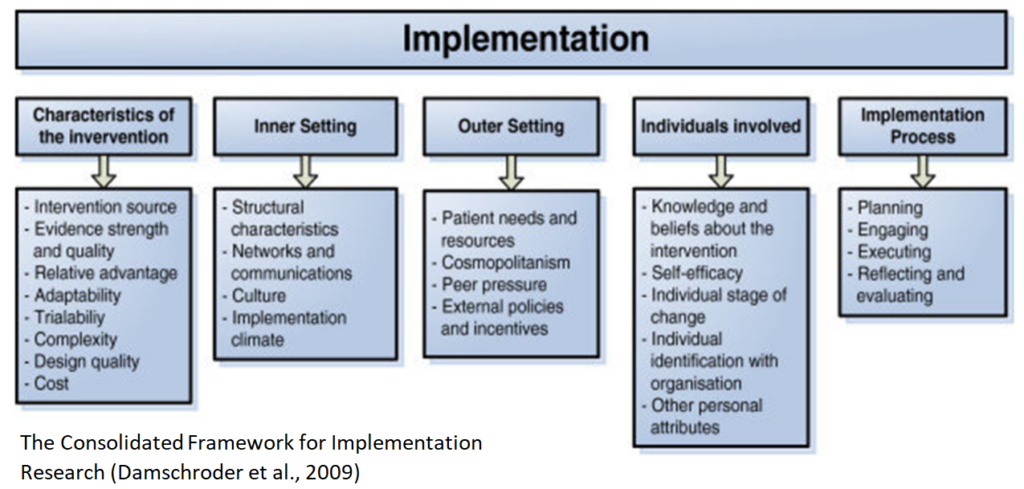
Out in the field it is useful for raising practitioners’ awareness and understanding of implementation and increases the chance they will make it a priority. Perhaps one of the most useful things implementation science allows me to do is help people understand what is helping or hindering implementation within their workplace. If we can work out what the biggest barriers and facilitators to implementation are then we can help them come up with an implementation plan to address these barriers. There are many implementation frameworks to help find out key barriers and facilitators which are often called ‘determinant frameworks’. But still the question remains how do you ‘do’ implementation?
Are Process frameworks the answer?
Within Implementation science I would say that ‘process frameworks’ are the closest thing to guidance on ‘how to’ implement. The Knowledge to Action Framework is the most cited of these (Field, Booth, Ilott, & Gerrish, 2014) and takes users through a series of steps in which they can address problems in healthcare by finding and moving appropriate knowledge into practice.
One of its key strengths is its awareness to be responsive to facilitating practitioner preferences and context-specific needs. A problem is discovered and knowledge to help it is searched for in the literature then adapted to the local context. Barriers and facilitators are assessed, and an appropriate course of action is then selected. Staff training is a common one.
These types of frameworks are very academic and require practical knowledge to bring them alive to really make a difference to the success of the implementation. And perhaps this is implementation science’s greatest challenge – how to bring its theories and frameworks to life, how to actually ‘do’ implementation. Because up until now it has tended to focus a great deal on understanding the problems of implementation rather than on understanding practical ways to address those problems. This gap between implementation science and implementation practice has been mentioned elsewhere (Moore, 2020). But why might this be the case? And what does this mean when it comes to actually supporting implementation? I decided to go on a journey to find out.
Surely, I thought, if I am to be an implementation specialist worth their salt, I need to be clear about ‘how to’ implement! I started interviewing implementation experts on my podcast Essential Implementation last year – To find out what I learnt be sure to check out Part 2 of this blog series: “Digging deeper – What I learnt from implementation experts!” You can also watch the interviews via the podcast link below.
Laura Damschroder – Implementation strategies for real life – YouTube
Contact for more information:
Kristian Hudson (Kristian.hudson@yhia.nhs.uk)
Implementation Specialist at the Improvement Academy
Bradford Institute for Health Research
I work at the Improvement Academy in Yorkshire, England, UK. We are a team of implementation scientists, improvement scientists, patient safety experts and clinicians who work with frontline services, patients and the public to deliver real and lasting change. Check out our website at https://improvementacademy.org/